CME speaker notes pancreas
Speaker notes pancreas


Slide 2:
• 50 Year old male came with complaints of :
• Abdominal distension with pain abdomen since 1 week
• Loss of appetite since 1 week
• Shortness of breath since 1 week
• B/L lower limb swelling since 5 days
• Decreased urine output since 5 days
HOPI
• Patient was apparently asymptomatic one week back then he noticed abdomeninal distention which was diffuse associated with abdominal pain( squeezing type ) not associated with vomotings, loose stools, fever Aggravated with food intake
• Complaints of bilateral pedal edema which is pitting type gradually progressive, extending from ankle to knee joint
• C/o decreased urine output and yellowish discolouration of urine since 5 days not associated with fever with chills and burning miturition, frothing of urine
• Complaints of shortness of breath with grade Il which is decreased in supine position
• No h/o chest pain, palpitations, excessive sweating.
• No H/o hematemisis, melena

Slide 3:
PAST HISTORY
• History of dengue 3years ago for which he was hospitalized for 15 days
• History of jaundice 2 years ago after which he was transfusions 2 prbc no records available
• No similar complaints in the past
• no history asthma.epilepsy, thyroid disorders, TB
• No history of previous surgeries

Slide 4:
PERSONAL HISTORY and DAILY ROUTINE
He is a government servant ,field worker in revenue department who wakes up at 5 am completes his daily routine and goes to work but most of the times he skips his breakfast. Eats lunch in between 2 - 4 pm because of his busy schedule and goes to bar at 6 pm to drink alcohol daily (whiskey 180 ml) and then goes home and eats dinner at 8pm and sleeps by 10 pm.
• DIET: mixed
• APPETITE: Decreased
• BOWEL MOVEMENTS: normal
• Bladder movements: decreased urine output since 5 days
• SLEEP : adequate
• Addictions: Alcoholic since 12 years,he used drink 180 ml of whiskey twice a week but from last 6 years he began drinking 180 ml of whiskey daily
• Last intake of alcohol was 15days ago

Slide 5
General examination
Patient was conscious, coherent cooperative
• Moderately build and moderately nourished
• Pallor: present
• Pedal oedema + pitting type
• No icterus, clubbing,cyanosis lymphadenopathy
• Vitals at admission:
• Temp: afebrile
• BP: 110/90 mmHg
• Pulse: 90 bpm
• RR: 22cpm
• Spo2: 98%
• GRbs 101 mg/dr
• Alopecia+
• No parotidomegaly
• No spider naevi
• No palmar erythema
• Dilated superficial abdominal veins +
• No testicular atrophy
• • No gynecomastia

Slide 6:
SYSTEMIC EXAMINATION
• Per abdomen:
• Ora cavity normal
INSPECTION:
• Shape:Distended
• Umbilicus:inverted, central
• Skin over the abdomen is shiny
• All quadrants are moving equally with respiration
• No visible peristalsis, Hernial orifices intact
• Visible superficial abdominal vein running vertically down is seen
• External genitalia normal
Palpation:
• Temperature:Not raised
• Tenderness+ in epigastrium
• No guarding rigidity
• Harvey's sign: flow of blood away from umbilicus above the level of umbilicus and below the level of umbilicus
• No hepatospleenomegalv
Percussion
Shifting dullness +
No fluid thrill
Puddles sign -not elicited
Liver span-12cm
Auscultation
Bowel sounds+
No arterial bruit. venous him
External genitalia:No loss of testicular volume or sensations
Respiratory system:
Inspection
• Shape of chest: Bilaterally symmetrical, Elliptical in shape
• No visible chest deformities
• No kyphoscoliosis,
• Abdomino thoracic respiration, No irregular respiration
• No tracheal shift
• No dropping of shoulders, Spino scapular distance appears equal on both sides no sinuses scars engorged veins
Palpation:inspectory findings confirmed by Palpation
• Chest movements -normal
Percussion:
Resonant note heard over all areas except infraaxillarv and intrascapular
Auscultation:
Norma vesicular breath sounds, Crepts+ in B/L infraaxillarv, infrascapular areas
Cardiovascular system: Inspection:precordium normal, apex beat :5th ICS half inch medial to mid clavicular line
Palpation:inspectory findings confirmed, No thrills or parasternal heave
Auscultation: S1S2+, no murmurs
CNS:HM normal, cranial nerves intact, motor and sensory examination normal
No cerebellar or meningeal signs

Slide 7:
PROVISIONAL DIAGNOSIS
Ascites secondary to chronic liver disease with
?Spontaneous bacterial peritonitis
?Pancreatitis


Slide 8,9,10,11,12:
Investigations
Ecg showed normal sinus rhythm
Echo showed Good LV function with EF 62%
Chest x ray was normal
Usg abdomen showed altered echo texture of liver with surface irregularity with moderate ascites likely chronic liver disease
Blood investigations and ascitic fluid reports will be read out as shown in the slides

Slide 13,14,15
With these clinical findings reports in hand we suspected it to be acute pancreatitis with underlying chronic liver disease .
He underwent CECT abdomen.
Which was reported as
• Gross ascites with diffuse omental haziness
• Uncinate process of pancreas showing mild heterogenous enhancement with peripancreatic fat stranding & few parenchymal calcification - Suggestive of acute on chronic pancreatitis.
• Mild quadrate lobe hypertrophy wi mild irregular margins - features are suggestive of early Chronic liver parenchymal disease
• Left simple renal cyst.
Which will be discussed briefly by Dr.PRIYANKA final year radiology post graduate
I invite Dr.Priyanka to expand our knowledge on the CECT abdomen of this patient.
Slide 13,14,15:By priyanka
……….
Thank you for the valuable inputs Priyanka

Slide 16:
Gastroenterology referral was taken an we suspected him to have pancreatic fistula as ascitic fluid amylase is more than 3 times the serum amylase and was referred to higher centre in view of need for ERCP
But as they did not get EHS for ERCP in private hospitals ,The patient was taken to government hospital in Hyderabad due to affordability issues ,where patient was put on Nasojejunal tube and position of tube confirmed by endoscopy as beyond D2 and therapeutic tap of 1.5 litres was done.
Follow up on call after 2 days:
Patient is now on naso jejunal feeds and is feeling better,his abdominal circumference has decreased.
Follow up on call after 15days:
Patient was discharged from outside hospital and was adviced for naso jejunal feeds and review ,2days after he was discharged patient had altered sensorium,patient was taken to the same hospital.He was intiated on CRRT yesterday in view of Acute kidney injury and is now fighting for his life currently.
Slide 17:My experience with pancreatic ascites

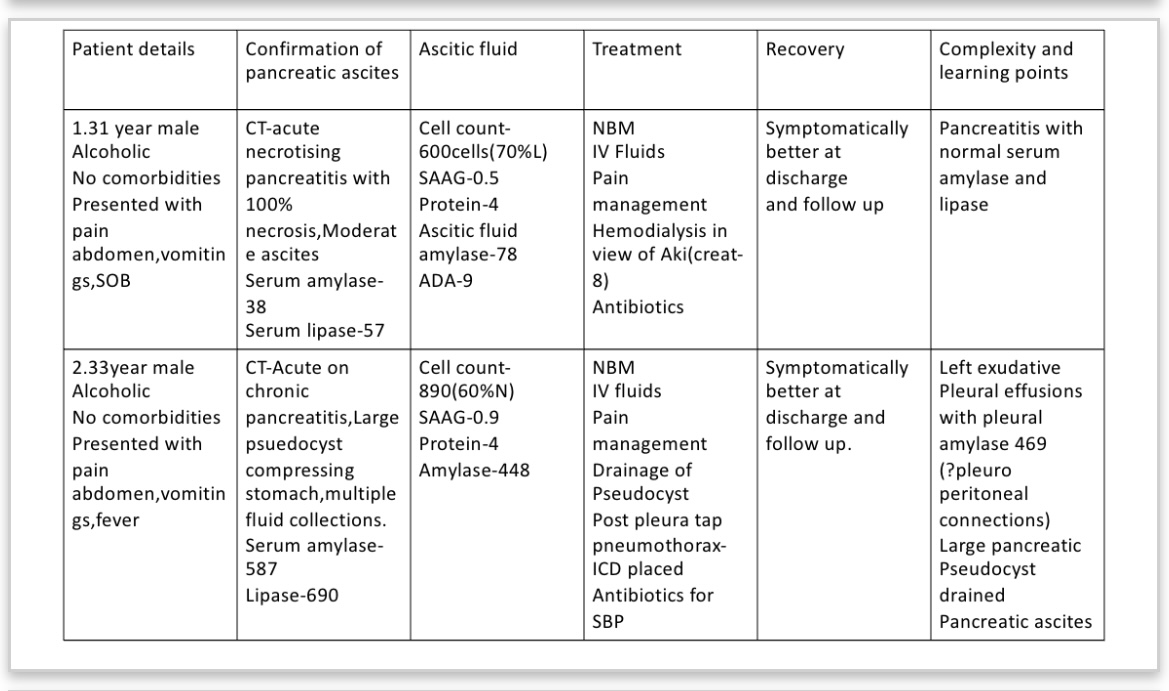


Slide 18 to 23 extra points to be added:
1.Pancreatitis with normal serum amylase lipase
2.Pleuro peritoneal connections
3.Pseudocyst of pancreas
4.Pancreatic fistula
5.Tubercular ascites vs pancreatic ascites



Comments
Post a Comment