70year male with multiple organ dysfunction
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Unit 1
Interns
Dr. Sravya Kandala
Dr. Navya
Dr. Raheem
Dr. Gnanadha
Dr. Chetana
Dr. Ashfaq
Dr. Charan PGY1
Dr. Chandana PGY1
Dr. Sushmitha PGY2
Dr. Adithya PGY3
Dr. Praneeth PGY3
Dr. Praveen Naik Ass. Prof.
Dr. RAKESH BISWAS HOD
Here is a case I've seen:
Admission under Unit 1 on 01/03/2021
75year old male shepherd by occupation apparently alright 3months ago ,non diabetic,non hypertensive,chronic smoker( since 40years,2chuttas/day),chronic alcoholic (since 40years 90ml/day)
Was brought to casualty on 1/2/2021 night with ET tube insitu on portable mechanical ventilator
On asking the attendors they give the history of
generalized edema 3months back (now subsided) pain abdomen(Rt sided) since 3days,anuria since 3days and constipation since 1day and was intubated outside in view of falling sats(spo2 40%)
On Reviewing outside hospital notes it was written as pt was brought in gasping state, unconscious state .Bp :NR,PR:40bpm and was intubated on 28/2/2021 in view of falling sats and was having MODS,AKI(outside last known creat on the day of intubation 3.6,urea 51) with severe life threatening metabolic acidosis(post intubation on SIMV on 28/2/2021 with Fio2 60% Ph 6.86,pco2 14.7,Hco3- 2.1,po2 342),on 1/3/2021 outside abg ph 7.35,pco2 26.8, hco3 14.7)outside ECG showed severe bradycardia (42bpm,regular)with junctional rhythm(absent p waves) ,low voltage complexes on chest leads(? secondary to COPD)
could be acute heart failure, myocardial depression secondary to severe metabolic acidosis
Outside CBP showed neurophilic leukocytosis(TLC 14,800,88% neutrophils) indicating some focus of sepsis
was treated outside with Iv antibiotics? unknown,iv fluids,iv steroids
outside ECG
severe bradycardia (42bpm,regular)with junctional rhythm(absent p waves) ,low voltage complexes on chest leads(? secondary to COPD)
outside chest x ray

DAy 1(1/3/2021)
When pt was brought to casualty
Pt is with ET tube insitu and on Ambu, conscious,moving all 4limbs
E4VTM6
Sats 99%
Bp 160/90
Grbs 115
PR 136bpm
JVP raised
his vitals were stable,no features of hypovolemia as written outside (resolved)
Foleys catheterization was done outside
Pt was connected to mechanical ventilator CPAP VC mode as abg showed Po2 retension (Ph7.1,pco2 50,hco3 16.0)
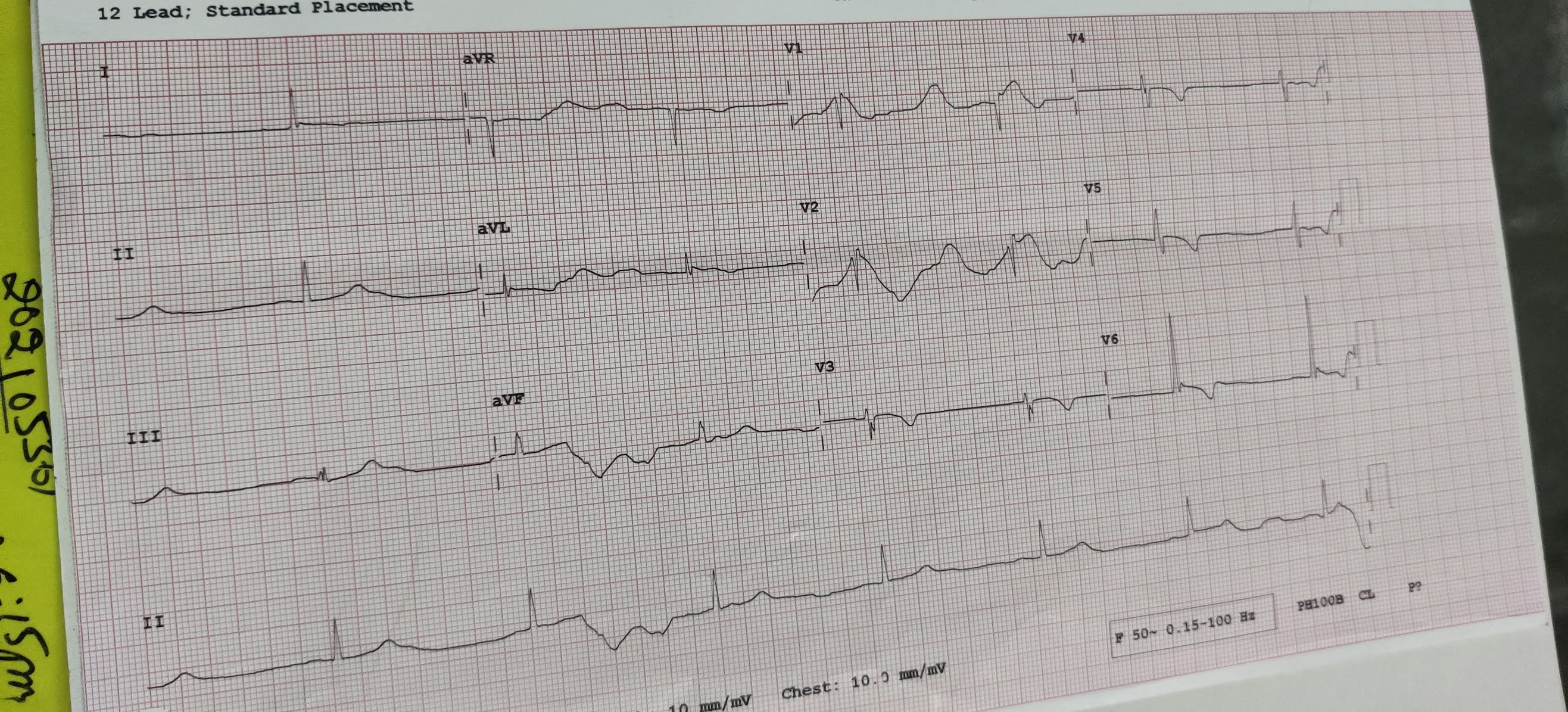
Ecg

chest x ray:AP view

With the history of Pain abdomen (right side),and constipation and sluggishness of bowel sounds differentials were made as
1.? intestinal obstruction followed by perforation and hypovolemic shock
2. ?acute appendicitis
3. ?uremic ileus
Usg abdomen:collapsed and aperistaltic bowel loops

DAY 2 (2/3/2021)
pt was slowly weaned off mechanical ventilation by 2/3/2021 afternoon
I/O 1500/1200
CUFF LEAK test
Before cuff leak

After cuff leak

This test consists of deflating the balloon cuff of the endotracheal tube to assess the air leak around the tube during expiration by measuring the expiratory tidal volume with and without a deflated cuff . A relatively large difference between these two values indicates that the cross-sectional area of the tracheal and/or upper airways is large enough to render the occurrence of post-extubation stridor, and therefore the possibility of re-intubation due to airway obstruction, unlikely
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1065107/#:~:text=The%20cuff%2Dleak%20test%20has,and%20without%20a%20deflated%20cuff.
post extubation Abg

After extubation pt was taken for chest x ray PA view

x ray erect abdomen
no features s/o intestinal obstruction

reports on day 1 and day2

Aditya Sir Pg 3rd Yr: Everything is fitting in with Uremia causing ileus and pain abdomen.
Aditya Sir PGy3: Metabolic acidosis from AKI in the background of severe COPD explains his intubation.
The key here is what led to the AKI ? The hepatitic pattern is likely from congestive hepatopathy
DAY 3
70yr old with Multiorgan dysfunction syndrome
Acute kidney injury(maintenance phase ,urine output 800ml) secondary to ?Sepsis(Outside report of neutrophilic leukocytosis)
Worsesningg inspite of iv fluids and foleys indicating Renal AKI ,ruling out pre renal and post renal AKI
?Congestive hepatopathy secondary to acute heart failure which is secondary to severe high anion gap metabolic acidosis(resolved)
Chronic obstructive pulmonary disease

S-pain abdomen resolved, cough+, generalized weakness
O-Bp 130/70
PR 90
Cvs s1s2+
RS Abdominal breathing,reduced almost absent chest expansion obsereved
Barrel shaped chest
Harrisons sulcus
Accessory muscle hypertrophy at supraclavicular fossa
Pursued lip breathing
Pink puffer




?Nicotine stains on lips
CVS :Jvp not raised as seen at the time of admission
S1s2+,no murmurs
A-serial LFT's

Serial LFTs show decreasing AST,increasing ALT
Discussion on serial LFTs:Congestive hepatopathy
[3/4, 5:10 PM] Aditya Sir Genmed Pg 3rd Yr: Super. So at baseline the AST was higher than the ALT. ALP is normal and the bilirubin is only mildly elevated.
This suggests that it is a purely hepatitic pattern and not a cholestatic pattern.
Causes of Hepatitis can be broadly split into ITVHO - Infections, Toxins, Vascular, Hereditary and Other causes.
Infections are most often viral - Hepatitis A to E and EBV, CMV, HSV and VZV. The produce a very characteristic elevation of enzymes to usually 1500 to 2000 and with ALT > AST. The half life of ALT is 3 to 4 weeks while that of AST is about 1 to 2 weeks. So it's unlikely to be an infection causing thia
[3/4, 5:12 PM] Aditya Sir Genmed Pg 3rd Yr: Toxins - The most common cause of toxin is Alcohol. Other toxins include Drugs, particularly Phenytoin, Valproate, Paracetamol, Isoniazid, Pyrazinamide and so on. He hasn't taken any of these has he ?
Classically, the pattern with toxin mediated hepatitis is ALT>AST, except with alcohol, which shows AST>ALT.
Other unusual toxins are recreational drugs like Cocaine and Meth and also recreational mushrooms.
[3/4, 5:17 PM] Aditya Sir Genmed Pg 3rd Yr: Vascular - Ischemic Hepatitis, Congestive Hepatopathy and Acute Budd Chiari. Ischemic hepatitis is a forward flow failure and involves zone 1 to 3 of the Rappaport zones in the hepatic lobules of the liver. If zone 1 is involved, they could have a clinically significant feature - Hypoglycemia and Lactic Acidosis (hence why these are classically seen in Malaria) both of which appear to be absent in this patient. Also Ischemic Hepatitis is one of the only cause where the enzymes may rise as high as 5000s. Also, they should have a history of HFrREF, neither of which the patient has.
Congestive Hepatopathy - Due to increased right sided heart pressures causing liver congestion. The enzymes in such a situation increase from anywhere between 20 to 30 fold of normal but almost always less than 1000.
Acute Budd Chiari is also very similar to congestive hepatopathy in terms of biochemical picture.
Importantly, all vascular causes show AST > ALT.
[3/4, 5:18 PM] Aditya Sir Genmed Pg 3rd Yr: Hereditary - Wilson's, Hereditary Hemochromatosis, Alpha 1 AT Deficiency. Flatly ruled out.
[3/4, 5:19 PM] Aditya Sir Genmed Pg 3rd Yr: Other causes - NASH, Autoimmune Hepatitis, Sickle Cell disease and quite common is Herbal Medicine use. Which can be considered a toxin too. Herbal medicine too produces a dramatic elevation of enzymes to levels of upto 2000 to 3000, on par with Viral Hepatitis.
[3/4, 5:19 PM] Aditya Sir Genmed Pg 3rd Yr: @Dr.Chandana Vishwanatham What is your provisional diagnosis now ?
[3/4, 6:08 PM] Dr.Chandana Vishwanatham: Congestive hepatopathy?
[3/4,6:010PM]Aditya sir:Seems so to me too
Worsesning AKI with urea 220,Creat 8.3, Electolytes within normal limits
P -pt attendors were counselled about need for dialysis but they denied,did not give consent and want to continue on conservative management
2d Echo was done



Diagnosis
70yr old with Multiorgan dysfunction syndrome and ?DIC secondary to ?sepsis
Acute kidney injury-Renal(maintenance) secondary to ?Sepsis(Outside report of neutrophilic leukocytosis)
?Congestive hepatopathy secondary to acute heart failure which is secondary to severe high anion gap metabolic acidosis(resolved) or ? Ischemic hepatitis secondary to shock
Chronic obstructive pulmonary disease



Comments
Post a Comment